Doxazosin vs Alternatives: Benefits, Side Effects & Cost Comparison
A detailed comparison of Doxazosin with its main alternatives, covering uses, side effects, costs, and when each drug is the best choice.
When looking at alternatives to Doxazosin, the range of medicines that can replace Doxazosin for treating high blood pressure or an enlarged prostate. Also known as Doxazosin substitutes, they help patients avoid specific side effects while still controlling the same conditions.
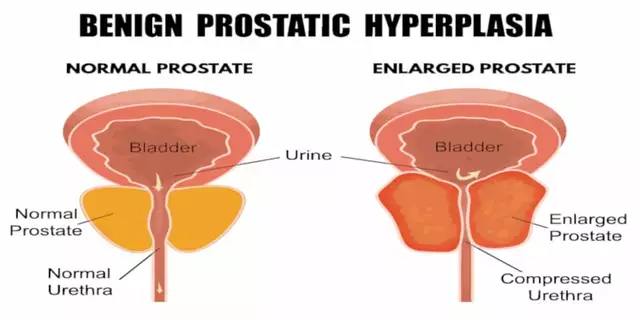
The original drug, Doxazosin, an alpha‑1 blocker prescribed for hypertension and BPH, belongs to the broader class of alpha‑blockers, agents that relax smooth muscle in blood vessels and the prostate. These agents are used to manage hypertension, a chronic elevation of arterial pressure that raises heart‑disease risk as well as Benign Prostatic Hyperplasia, non‑cancerous prostate enlargement that causes urinary difficulty. Because the same drug class touches both conditions, many patients wonder whether switching to a different member of the class or even to a completely different class might give better symptom control or fewer side effects. In short, alternatives to Doxazosin encompass a mix of other alpha‑blockers, drugs from other classes, and sometimes non‑pharmacologic approaches.
First, look at the drug’s selectivity. Terazosin and Prazosin are older alpha‑1 blockers that share Doxazosin’s blood‑pressure‑lowering ability but often cause more pronounced “first‑dose” dizziness. Tamsulosin, on the other hand, is highly selective for prostate‑rich receptors, which means it eases urinary symptoms with a lower impact on blood pressure—great for men whose main issue is BPH. If you need both blood‑pressure control and prostate relief, many clinicians pair a modest dose of Tamsulosin with a separate antihypertensive like an ACE inhibitor or a thiazide diuretic.
Second, consider side‑effect profiles. Doxazosin can trigger orthostatic hypotension, especially at night, and may cause fluid retention in some patients. Prazosin often leads to vivid dreams, a quirk that bothers a subset of users. Dutasteride and Finasteride are not alpha‑blockers but 5‑alpha‑reductase inhibitors; they shrink the prostate over months and completely sidestep the blood‑pressure effects of alpha‑blockers. For men who can tolerate a slower onset of action, these drugs are a solid alternative, especially if they already have a separate blood‑pressure regimen.
Third, think about drug interactions. Alpha‑blockers amplify the effect of other vasodilators such as nitrates or certain calcium‑channel blockers. When switching, a careful medication review helps avoid dangerous blood‑pressure drops. In patients taking erectile‑function drugs like sildenafil, Tamsulosin is generally safe, while non‑selective alpha‑blockers may increase the risk of priapism. This interaction map shows why a personalized review is crucial before making any change.
Finally, evaluate patient lifestyle. Some people prefer once‑daily dosing; Tamsulosin and Dutasteride fit that bill nicely. Others need flexible dosing because they miss a dose occasionally; shorter‑acting agents like Prazosin can be restarted quickly without a long washout period. The decision also depends on kidney function—certain beta‑blockers and ACE inhibitors may be less suitable for patients with advanced renal disease, pushing the choice toward a renal‑safe alpha‑blocker.
The collection below reflects these real‑world considerations. You’ll find detailed guides on how to talk to your doctor about Rivastigmine, why Losartan adherence matters, and how to compare serum lipid‑lowering options—all written with the same practical tone. Whether you’re hunting for a swap that eases dizziness, looking for a prostate‑focused medication, or need to pair an alpha‑blocker with another antihypertensive, the articles ahead break down the evidence, side‑effects, and cost factors you’ll need to decide. Dive in to get a clearer picture of what works best for you and to pick the safest, most effective alternative.
A detailed comparison of Doxazosin with its main alternatives, covering uses, side effects, costs, and when each drug is the best choice.